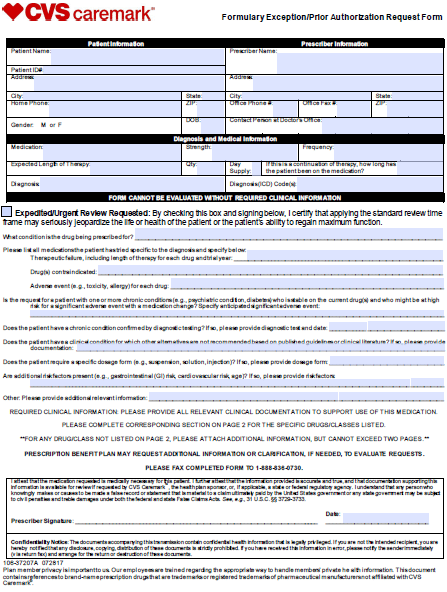
A physician will need to fill in the form with the patients medical information and submit it to CVSCaremark for assessment. Fax signed forms to CVSCaremark at 1-888-836-0730.
 Top Cvs Caremark Prior Authorization Form Templates Free To Download In Pdf Format
Top Cvs Caremark Prior Authorization Form Templates Free To Download In Pdf Format
Fax signed forms to CVSCaremark at 1-888-836-0730.
Cvs caremark authorization form. The CVScaremark app lets you manage your prescription benefits on the go. Print Plan Forms Download a form to start a new mail order prescription. Our electronic prior authorization solution ePA is hipaa compatible and is available for all plans and medicines at no cost to suppliers and their staff.
If you wish to request a Medicare Part Determination Prior Authorization or Exception request please see your plans website for the appropriate form and instructions on how to submit your request. Insurance policies have their limitations and in some cases a physician must complete and submit the SilverScript prior authorization form in order to get approval for the drug they intend to prescribe to their patient. CVS Caremark will review and provide authorization for specialty drug requests on our behalf.
Prescription Drug Prior Authorization Form - CVSCAREMARK. A SilverScript prior authorization form is required in order for certain drug prescriptions to be covered by an insurance plan. Permission from CVS Caremark.
1 PRIOR AUTHORIZATION CRITERIA BRAND NAME generic diclofenac sodium gel 3. Ormulary ExceptionPrior Authorization Request Form Patient Information Prescriber Information Patient Name. Completereview information sign and date.
Cvs caremark prior authorization form for xeljanz CoverMyMeds is the fastest and easiest way to review complete and track PA requests. Completereview information sign and date. CVSCaremark Prior Authorization Form California Created Date.
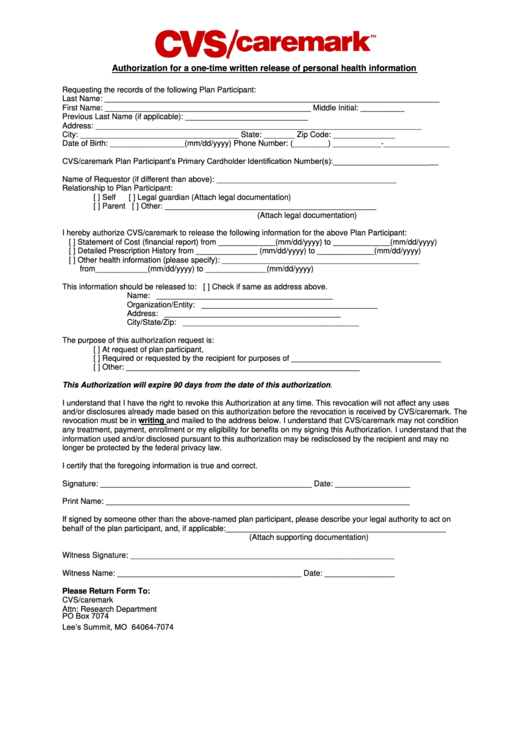
I understand that signing this authorization is voluntary and that this authorization will not. Cvs caremark prior authorization form for otezla When a PA is required for a prescription members will be asked to have the doctor or the doctors authorized agent contact our Prior Authorization Department to answer the question criteria for determining coverage. Privacy Office One CVS Drive Woonsocket RI 02895 or fax to 401-765-9304 except to the extent that CVS Pharmacy has taken action in reliance on this authorization.
Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process. Completereview information sign and date. Prior Authorization Form Opana ER This fax machine is located in a secure location as required by HIPAA regulations.
Formulary ExceptionPrior Authorization Request Form Patient Information Prescriber Information Patient Name. Prior Authorization Form Namenda This fax machine is located in a secure location as required by HIPAA regulations. Fax signed forms to CVSCaremark at 1-888-836-0730.
Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process. Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process. Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process.
This document contains references to brand-name prescription drugs that are trademarks or registered trademarks of pharmaceutical manufacturers not affiliated with CVS Caremark. Prior Authorization Form Duragesic This fax machine is located in a secure location as required by HIPAA regulations. Brand-name prescription drugs that are trademarks or registered trademarks of pharmaceutical manufacturers not affiliated with CVS Caremark.
Prior Authorization Form Razadyne This fax machine is located in a secure location as required by HIPAA regulations. Completereview information sign and date. The CVSCaremark prior authorization form is to be used by a medical office when requesting coverage for a CVSCaremark plan members prescription.
Select the Provider tab Tools Resources then Forms. CVSCaremark Prior Rx Authorization Form. Prior Authorization Form Isotretinoin Products This fax machine is located in a secure location as required by HIPAA regulations.
Drug Reference Interactions. Contains references to brand-name prescription drugs that are trademarks or registered trademarks of pharmaceutical manufacturers not affiliated with CVS Caremark. Fax signed forms to CVSCaremark at 1-866-217-5644.
To manage your prescriptions sign in or register. Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process. Completereview information sign and date.
Please contact CVSCaremark at 1-800-294-5979 with questions regarding the prior authorization process. Prior Authorization Form Strattera This fax machine is located in a secure location as required by HIPAA regulations. Contact CVS Caremark Prior Authorization Department Medicare Part D.
Fax signed forms to CVSCaremark at 1-888-836-0730. Fax signed forms to CVSCaremark at 1-888-836-0730. Completereview information sign and date.