For patients currently on Xolair for the treatment of chronic urticaria authorization for continued use will be approved based on all of the following criteria. Fax - 1-855-476-4158.
 Fillable Online Prior Authorization Form Prior Authorization Form For Medicare Plan Part B And Part D Fax Email Print Pdffiller
Fillable Online Prior Authorization Form Prior Authorization Form For Medicare Plan Part B And Part D Fax Email Print Pdffiller
XOLAIR Prior Authorization Form WVDRGSPA-108 Page 2 of 2 Rev03302011 omalizumab 6.
Xolair prior authorization form. Xolair Prior Authorization Request Form Page 1 of 2 DO NOT COPY FOR FUTURE USE. OptumRx has partnered with CoverMyMeds to receive prior authorization requests. Section A Member Information First Name.
Reside in the state of Colorado andor. Has the patient reacted positively to a perennial aeroallergen skin or blood test. Xolair PRIOR AUTHORIZATION REQUEST FORM Please complete this entire form and fax it to.
ONLY COMPLETED REQUESTS WILL BE REVIEWED. Who reside in the state of Louisiana andor. Louisiana uniform prescription drug prior authorization form PDF opens new window.
Whose prescription drug coverage was sold in the state of Louisiana. Obtain at MVPs specialty pharmacy CVS Caremark to be shipped to office for administration Circle. Please indicate how medication will be obtained.
XOLAIR omalizumab preferred PRIOR AUTHORIZATION FORM. Member Information required Provider Information required Member Name. Medication Prior Authorization scroll down the or center of the page to find a.
Xolair PharmacyPrior Authorization Request Form. Omalizumab Xolair Injectable Medication Precertification Request All fields must be completed and legible for precertification review Aetna Precertification Notification 503 Sunport Lane Orlando FL 32809 Phone. Fax completed prior authorization request form to 877-309-8077 or submit Electronic Prior Authorization through CoverMyMeds or SureScripts.
The use of this form is mandated for prior authorization requests concerning commercial fully insured members. Prior Authorization can ensure proper patient selection dosage drug administration and duration of selected drugs. Office drugs prior authorization request PDF 301 KB.
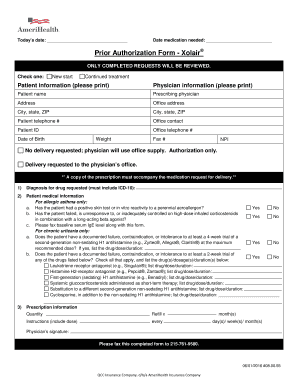
I am a board certified pulmonologist or a board certified Date of test7. Prior Authorization Form Xolair Buy-and-bill requests for this drug should be submitted through NaviNet. Monoclonal Antibodies Anti-Il Anti-IgE.
This patients benefit plan requires prior authorization for certain medications in order for the drug to be covered. Xolair HMSA - Prior Authorization Request CVS Caremark administers the prescription benefit plan for the patient identified. PRIOR AUTHORIZATION FORM Xolair omalizumab for asthma Dose Frequency _____ Diagnosis.
Form effective 050119. Quantity LimitsDaily Dose Limits. M New start M Continued treatment Patient information please print Physician information please print Patient name Prescribing physician Address Office address.
All requests for Xolair omalizumab require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Fax completed prior authorization request form to 855-296-0323 orsubmit Electronic Prior Authorization. Allow at least 24 hours for review.
Will the patient be using Xolair in combination with other biologic medications for. This form contains multiple pages. O Documentation of positive clinical response eg reduction in exacerbations itch severity hives.
If you have questions please call 800-310-6826. Weve provided the following resources to help you understand Anthems prior authorization process and obtain authorization for your patients when its required. Prior Authorization Health insurance can be complicatedespecially when it comes to prior authorization also referred to as pre-approval pre-authorization and pre-certification.
Xolair omalizumab Created Date. Submit the Registration form with a completed Medication Authorization Request Form MARF via fax or mail. To make an appropriate determination providing the most accurate diagnosis for the use of the.
Please complete all pages to avoid a delay in our decision. Standard Drug Request Form PDF 428 KB Topical Antihistamines PDF 462 KB Topical Anti-Inflammatory PDF 461 KB Topical Local Anesthetics Lidoderm Patch lidocaine patch and ZT Lido PDF 456 KB Triptans PDF 458 KB Vusion PDF 488 KB Xenazine and tetrabenazine for Movement Disorders PDF 465 KB Xolair PDF 622 KB Zolgensma PDF 556 KB. Officen otes labs and medical testing relevant to request show ingmedical justification are required tos upportd.
Prior Authorization Form for Xolair. Xolair PSC Prior Authorization Form Author. PA Forms for Physicians When a PA is needed for a prescription the member will be asked to have the physician or authorized agent of the physician contact our Prior Authorization Department to answer criteria questions to determine coverage.
FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED. Illinois authorization request form. Prior AuthorizationCoverage Determination Form PDF 136 KB Prior Authorization Generic Fax Form PDF 173 KB Prior Authorization Urgent Expedited Fax Form PDF 126 KB Tier Exception PDF 109 KB Prescription drug prior authorization and step therapy exception request forms.
Formsa reu pdatedf requently. Prior authorization guidelines for. Whose prescription drug coverage was sold in the state of Colorado.
Donotc opyf orf utureu se. The use of this form is mandated for prior authorization requests concerning commercial fully insured members who. Prescription drug prior authorization request form PDF opens new window.
 Fillable Online Prior Authorization Request Form For Fax Email Print Pdffiller
Fillable Online Prior Authorization Request Form For Fax Email Print Pdffiller
Https Static Cigna Com Assets Chcp Pdf Resourcelibrary Prescription Xolair Pdf
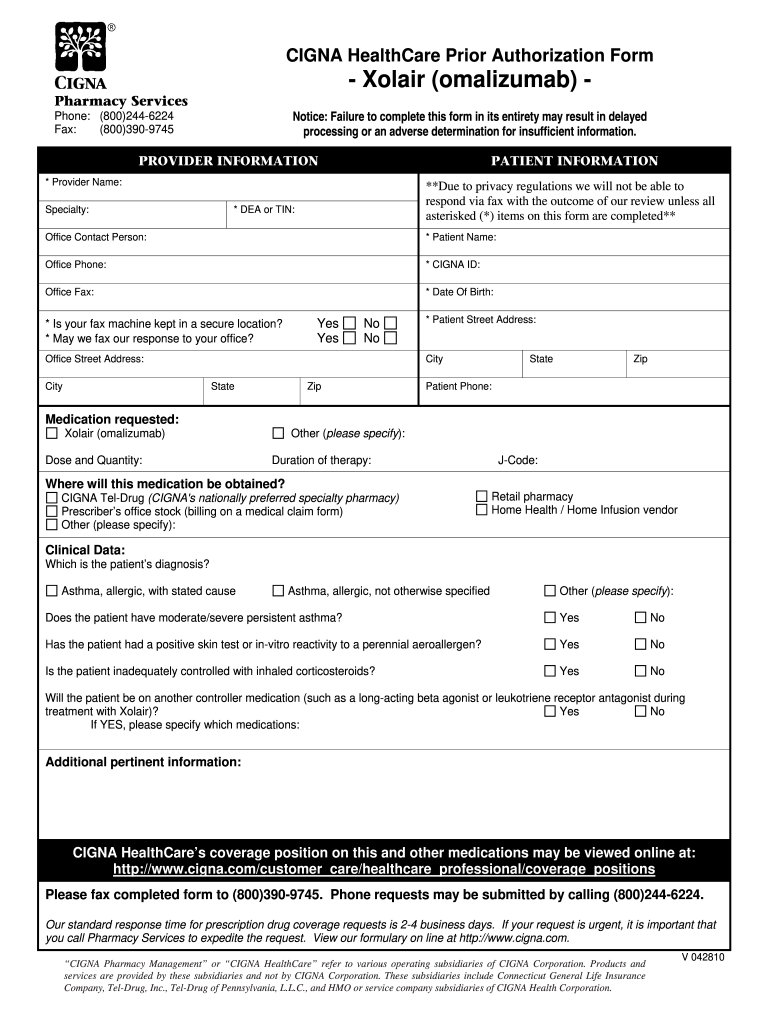 Cigna Xolair Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Cigna Xolair Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Https Www Keystonefirstpa Com Pdf Pharmacy Forms Injectable Xolair Pdf
 Cigna Xolair Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Cigna Xolair Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
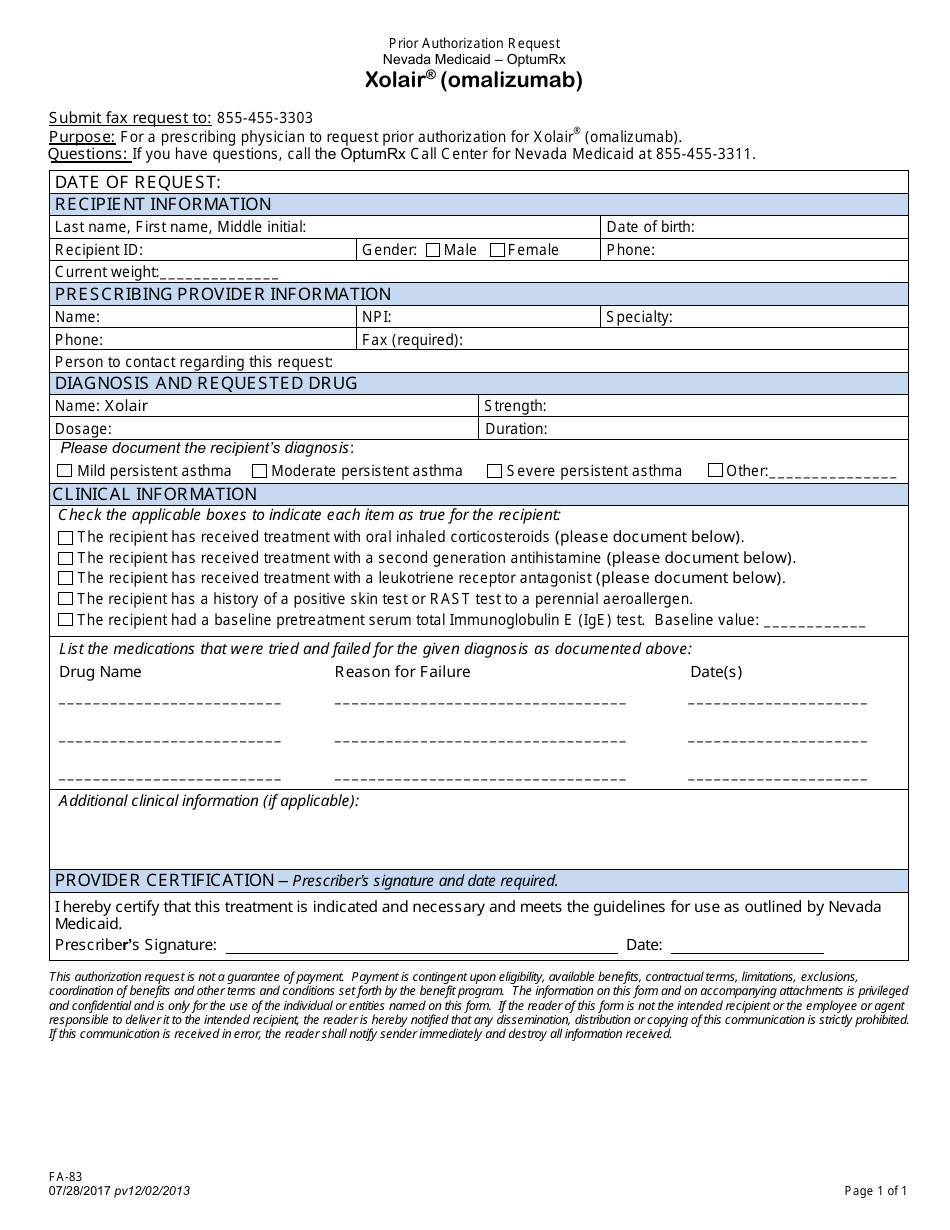 Form Fa 83 Download Fillable Pdf Or Fill Online Prior Authorization Request Xolair Omalizumab Nevada Templateroller
Form Fa 83 Download Fillable Pdf Or Fill Online Prior Authorization Request Xolair Omalizumab Nevada Templateroller
Https Www Bluecrossnc Com Document Providers Public Pdfs Xolair818pdf
 Fillable Online Care Prior Authorization Form Plus Fax Email Print Pdffiller
Fillable Online Care Prior Authorization Form Plus Fax Email Print Pdffiller
Https Www Uhcprovider Com Content Dam Provider Docs Public Prior Auth Uhccp Pharmacy Forms U Z Upc Xolair Prior Auth Form Pdf
Https Www Bcbsil Com Pdf Pharmacy Xolair Pdf
 Xolaira Prior Authorization Form Dhhr
Xolaira Prior Authorization Form Dhhr
2
 Fillable Online Prior Authorization Form If This Is An Urgent Fax Email Print Pdffiller
Fillable Online Prior Authorization Form If This Is An Urgent Fax Email Print Pdffiller
Http Www Aetna Com Pharmacy Insurance Healthcare Professional Documents Xolair Precert Form Pdf




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.